|
Startseite
© 2018 Dr. Graumann-Brunt |
|||
Chewing, speaking and the pterygoidei muscles © Dr.Sigrid Graumann-Brunt In the practice of speech therapy one quite often encounters patients that have a problem chewing solid food. It is no coincidence to find such patients in the speech therapy room because speech motor problems often go hand in hand with difficulty chewing. And not without good reason, as it has been known for some time that elements of the chewing pattern are to be found in speech-related movements ( see Fröschels: in addition to the opening and closing of the mouth, the forward and backward motion of the lower jaw are common to both patterns). However, the movements common to both speech and chewing are by no means identical; there are differences, e.g. the angle at which the jaws are opened for the purpose of speaking differs from that required for the act of chewing and the teeth are set further apart; moreover, the mouth is generally closed when chewing. We can, nevertheless, still assume a certain degree of similarity and it is therefore worth taking a closer look at the act of chewing while bearing in mind the movements observed in the act of speaking. The temporomandibular joint is a minor technical miracle because it enables us to open our mouth wide, close it, but also to move the lower jaw forwards and back again. The opening and forward motions combined give rise to a shovel-like movement. Perhaps it was this that first gave us the idea for the shovel excavator. The muscles involved in the act of chewing can be quite clearly seen. They are - the musculus temporalis (1) ( provides the necessary pressure for chewing and pulls back the lower jaw.) and - the musculus masseter (2) ( provides the necessary pressure for chewing), 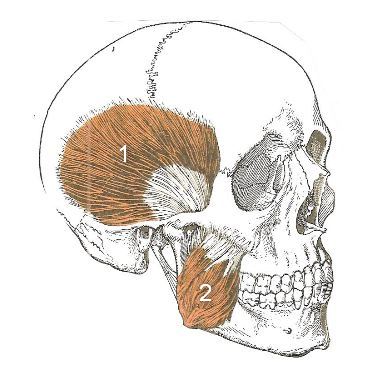
- the musculus pterygoideus lateralis (3) (pulls the lower jaw forward) and - the musculus pterygoideus mediales (4) (contributes to the pressure necessary for chewing) 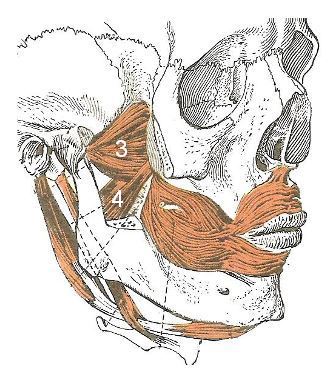
taken from Lippert: Anatomie. Text und Atlas, 10th edition 2017 copyright Elsevier GmbH, Urban & Fischer, Munich (We cannot accept any liability for any claims lodged by third parties) The first three above-mentioned muscles are particularly strong; they all play a part in closing the mouth and in providing the pressure necessary for chewing. The functional mechanics of chewing will be readily understood by those who tinkering with mechanical devices, but everyone else will need to acquire a certain "feeling" for it. Beginning with the musculus temporalis, where one needs to distinguish between its twin functions: the anterior parts perform the same function as the musculus masseter (exerting pressure for the act of chewing) whereas its posterior sections perform something quite different in that they pull the lower jaw back. Its opposite number in this respect, the muscle that pulls the lower jaw forward, is the musculus pterygoideus lateralis. Movement patterns The mouth is opened by the action of the musculus pterygoideus lateralis pulling the condyle of the lower jaw out of the mandibular fossae in a forward movement. A number of further ligaments, omitted here for the sake of simplicity, hold the lower jaw firm as they pull down. The lower jaw is pushed forward by the pulling action of the musculus pterygoideus lateralis while the masseter and the musculus pterygoideus medialis prevent the jaw from opening. The retraction of the lower jaw is performed by the lower sections of the musculus temporalis; this, however, requires restraining the action of the musculus pterygoideus lateralis. So far, so good; but the grinding action of chewing is not, unfortunately, a synchronous parallel pattern of movement; on the contrary, it is a counterdirectional one (comparable perhaps to the act of locomotion, which, once fully developed, necessitates a cross-pattern movement). This means that, during the grinding action of chewing, the lower jaw swings back and forth alternately to the left and right. This action is produced by the temporomandibular joint being pulled forward on one side and backwards on the other. Earlier and later patterns This cannot be achieved unless earlier patterns of movement in which the left and right parts of the mouth move synchronously in parallel fashion cease to dominate. If the suck reflex still persists and becomes active, it will cause "interference". In such cases work will need to be done to mitigate the persisting suck reflex (with eyes closed!). When one considers the complexity of these patterns of movement, it is hardly surprising that they are prone to impairment and that complaints of insufficient chewing become audible in the therapy room. The lower jaw may not have grown sufficiently in size and strength (at birth it is very small by comparison and does not need to acquire more "mass" until sucking is superseded by chewing). The angle to which the jaw opens may not be wide enough, the lower jaw may have insufficient or no forward thrust, etc. (see also Angermann´s convincing observations from the behavioural biologist´s point of view that suggest that the lower jaw.can and may only be thrust forward and interpreted as a social gesture from a certain age or stage of development). If one takes conditions in the cranial muscles into account, which one is well advised to do as far as possible, it becomes clear that the complex function of the musculus temporalis in particular may be severely impaired by a general tenseness in the cranial region. A psychological aspect may also, of course, play a part in the problem: everyone knows of the need to "clench one´s teeth" in critical situations – a tensing of all muscles. Asymmetry factors are often found among the complex of symptoms, as they tend to be particularly evident in the temporomandibular joint, and then it is not only the forward thrust which "jams". It is often accompanied by a persisting tonic labyrinthine reflex which hinders manoeuvring of the lower jaw.(see the diagrams illustrating the position of the lower jaw in the lecture on stuttering). Whatever the genesis of these asymmetry factors may be, they indirectly impair the act of chewing and speaking, do damage to the joints and muscles and may result in a rejection of coarser forms of nutrition. Work on asymmetry of this kind is therefore fundamentally beneficial; to put it more precisely, it is one of the cornerstones of therapeutic treatment. There are, however, one or two very simple but useful tips that may help: Massage the musculus temporalis and practise tensing and relaxing it (front and rear region of the musculus temporalis. It is usually quite easy to locate and touch with the fingers. Massage all head muscles to relax them (like any good hairdresser is capable of doing), a treatment generally much appreciated by all. You can have the child feel for what is called the head joint ( located the width of one finger above the wing of sphenoid bone, adjacent to the temporal bone, a region where tension is often present, and allow the child to gently massage the spot. The musculi pterygoidei are frequently tense to the point of causing pain. Children are quite able to relieve tension in these muscles by applying their index finger to the inside of the mouth (another finger applied to the same place on the outside of the face in the vicinity of the ear can aid orientation). Problems concerning the structural equilibrium of the body as a whole and the posture of the head have been omitted here for the sake of simplicity. The same applies to some further aspects, including the fact that, despite its bony constitution, the mandible is not merely functional, but should, from a genetic perspective, be assigned to the digestive system (see claims made by embryologists as to their developing from a common somite) and that there may be a connection between digestive disorders and dysfunctions in the mandible´s movement patterns. The production of speech sounds has likewise been omitted, although it would be interesting to investigate evidence of the "grinding" action playing a part in speech motor patterns (when forming the sch sound in German maybe?). This would be taking matters too far here. I should like to thank the publishers, Elsevier, very much for granting me permission to use illustrations from Lippert´s book (which I can sincerely recommend to everyone) |

